9300 - Delirium
DBQ: Link to Index of DBQ/Exams by Disability for DC 9300
Acronym: DELIR
Definition
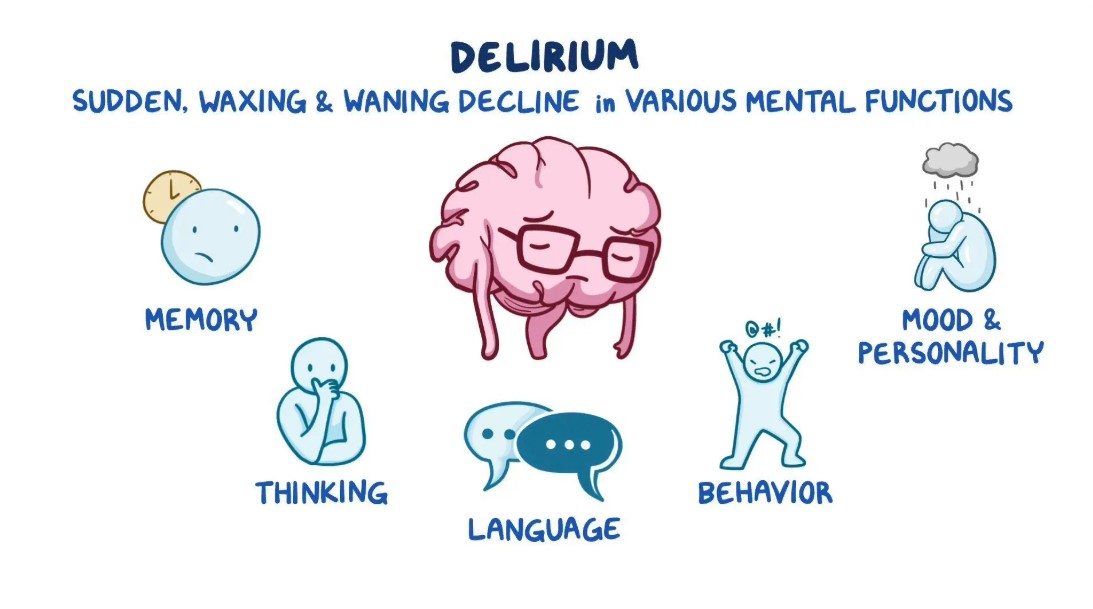
A mental state that arises rapidly and is marked by a change in cognition. There is impairment in attention span and memory, disorientation to time and place, and the distortion of perception may give rise to illusions or hallucinations or both.
{kind=link}
Etiology
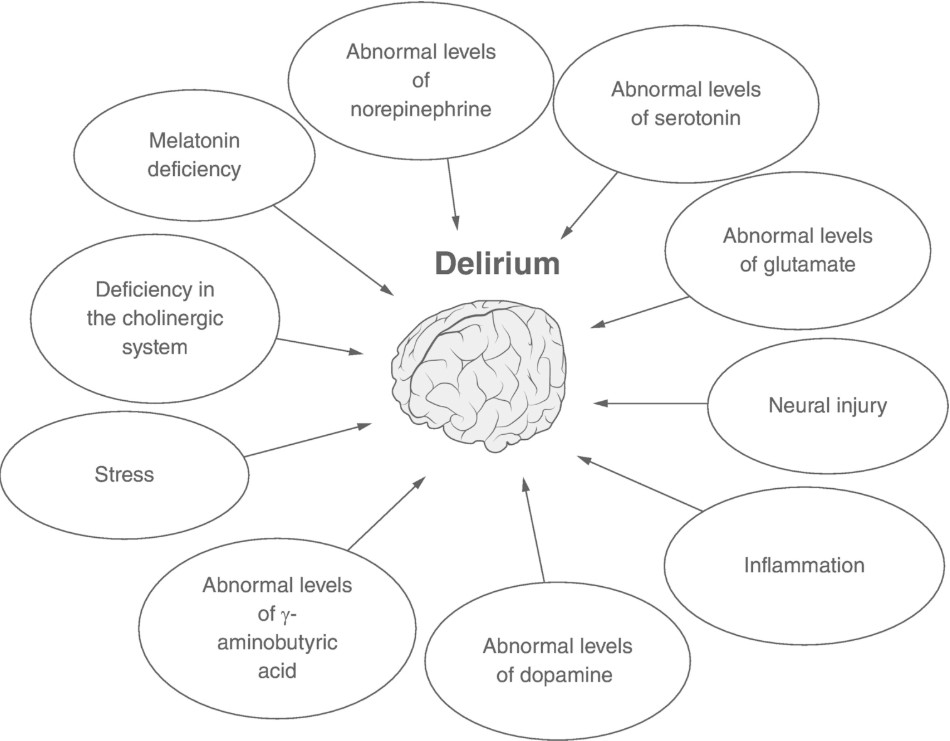
Some common causes of the condition include:
{kind=link}
-
Metabolic related to any metabolic disorder, which can cause delirium.
-
Toxic related to drug reactions or side effects, particularly in the elderly.
-
Structural related to vascular lesions, cerebral hemorrhage, brain tumors, and subdural hematomas.
-
Infectious related to fever-induced delirium, meningitis, encephalitis, pneumonia, and viral infections.
Signs & Symptoms
Symptoms vary within minutes, and become worse later in the day (sundown effect). There can be an increase in psychomotor activity or a decrease in activity. The consciousness is clouded, and disorientation to time, place, or person occurs. Sleeping and eating patterns are usually distorted. Emotional outbreaks may vary. Patients may demonstrate fear, apathy, euphoria, irritability, or anger.
{kind=link}
Tests
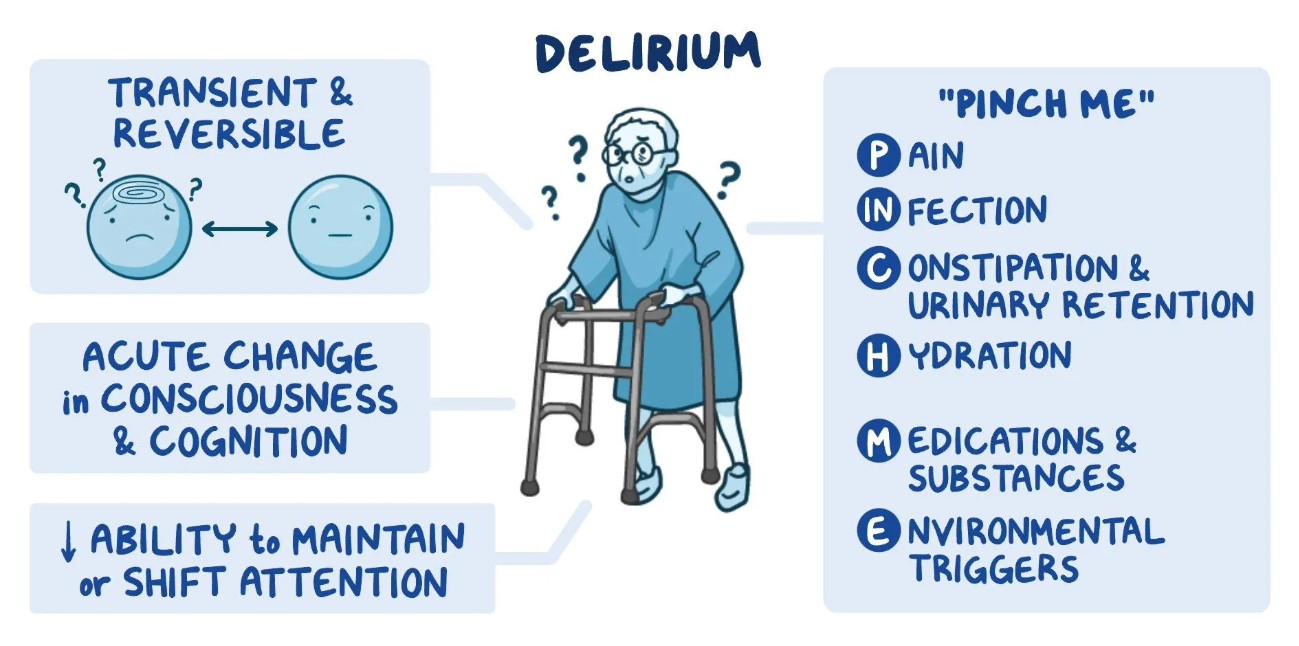
Differentiating delirium from dementia is necessary. Diagnostic criteria have been developed, and the diagnosis is made almost solely on clinical grounds. Laboratory tests are performed to search for medical causes of the delirium.
Treatment
This condition is reversible when the basis for the delirium is identified. Proper treatment and management is essential. Causes from drug toxicity, hypoglycemia, or infection can be treated. However, recovery in the elderly may be slow. A calm, quiet, lowly lighted environment will assist in decreasing over-stimulation. In most incidences, psychoactive drugs if needed for agitation, should be reduced and eliminated as soon as possible in order to evaluate non-drugged behavior.
Residuals
Prompt treatments of underlying causes make complete recovery a possibility.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
Competency must be addressed in cases where a mental condition is initially evaluated as totally disabling or when the total evaluation is continued in a rating decision. This includes when individual unemployability is awarded or continued on the basis of a single mental health disability, and when assigning or continuing a temporary total evaluation for a mental disorder under 38 CFR 4.29 [38 CFR 3.353 [Determinations of incompetency and competency]].
-
Reference 38 CFR 3.384 for the applicability of the term psychosis.
-
Review 38 CFR 3.354 with regard to determinations of insanit
Notes
-
An incapacitating episode is a period during which bed rest and treatment by a physician are required.
-
Ratings under diagnostic codes 9201 to 9440 will be evaluated using the General Rating Formula for Mental Disorders. Ratings under diagnostic codes 9520 and 9521 will be evaluated using the General Rating Formula for Eating Disorders.
-
Review the special provision outlined in 38 CFR 4.125 through 38 CFR 4.129 for decisions related to mental disorders.
-
The nomenclature employed in this portion of the rating schedule is based upon the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM–5) (see 38 CFR 4.125 for availability information). Rating agencies must be thoroughly familiar with this manual to properly implement the directives in 38 CFR 4.125 through 38 CFR 4.129 and to apply the general rating formula for mental disorders in 38 CFR 4.130.